

p (1).png)



.png)




.png)

Case Report
SEPTOCOLUMELAR SUTURE TECHNIQUE AS A NASAL TIP POSITIONING AND PRESERVATION METHOD
- Jorge Alberto Espinosa-Reyes, MD
Corresponding author: Jorge Alberto Espinosa-Reyes, MD, ENT, Facial Plastic Surgeon Calle 127a # 7- 53 cons 3005 (INO), Bogotá, Colombia, ORCID: 0009-0008-7673-586x
Volume: 1
Issue: 1
Article Information
Article Type : Case Report
Citation : Jorge Alberto Espinosa-Reyes MD, Luis Solís MD, Roxana Cobo MD, Nicolás Heredia-Combariza MD, Mauricio Puerta MD, Diego Corredor MD, Juan Carlos Ochoa Álvarez MD. Septocolumelar Suture Technique as a Nasal Tip Positioning and Preservation Method. Journal of Surgery Research 1(1). https://doi.org/10.61615/JSR/2025/SEPT027140924
Copyright: © 2025 Jorge Alberto Espinosa-Reyes, MD. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.61615/JSR/2025/SEPT027140924
Publication History
Received Date
02 Sep ,2025
Accepted Date
15 Sep ,2025
Published Date
24 Sep ,2025
Abstract
The septocolumellar suture technique is reliable for positioning and reshaping the nasal tip in rhinoplasty. This technique involves placing a loop suture between the medial crura and the caudal septum to maintain, increase, or decrease the projection and rotation of the nasal tip. Successful use of this technique requires proper preoperative analysis and consideration of the strength and position of the nasal septum. Grafts can be used for additional support and definition. The septocolumellar suture technique is valuable for achieving desired nasal tip aesthetics in rhinoplasty.
►SEPTOCOLUMELAR SUTURE TECHNIQUE AS A NASAL TIP POSITIONING AND PRESERVATION METHOD
Jorge Espinosa MD1*, Luis Solís MD2, Roxana Cobo MD3, Nicolas Heredia MD1, Mauricio Puerta MD2, Diego Corredor MD2, Juan C Ochoa MD2
1 ENT and Professor of Facial Plastic Surgery Fellowship – The Face & Nose Institute, Bogotá 110121, Colombia.
2 ENT and Facial Plastic Surgery Fellow – The Face & Nose Institute, Bogotá 110121, Colombia.
3ENT and Professor of Facial Plastic Surgery Fellowship – The Face & Nose Institute, Cali 760044, Colombia.
Introduction
The main goal of rhinoplasty has changed from looking for an aesthetically beautiful nose to a natural, attractive, and functionally suitable one. The form, rotation, and projection of the nasal tip give the base of a good result in rhinoplasty.[1] There are different methods to measure these parameters, and at the moment, there is no gold standard for any, but it is very important to be consistent with the method of measurement.[2] Most of the complications and unfavorable results in rhinoplasty come from the nasal tip subunit and are especially secondary to alterations in the medial crus and caudal septum proportions. The nasal tip must be considered the center of attention during a rhinoplasty procedure, which will guide the treatment for the other subunits of the nose.[3]
Previously, most techniques were performed by aggressive cutting and excising the nasal tip and alae. This resection often resulted in the loss of nasal tip support, with the risk of deformation and functional compromise. The techniques that involve sutures for the management of the nasal tip are not new; however, their use became more popular in the 80s, being more varied in techniques and contemplating different aspects of the nasal tip.[4] The techniques based on cartilage sutures are an alternative for the modification of the projection, rotation, and degree of thinning of the tip.[5,6]
For a rhinoplasty to be successful, a proper preoperative analysis must be performed, including a complete nasal examination and the analysis of digital photographs. In a frontal view, the face is usually divided into three equal thirds, and the evaluation of each one is important to diagnose important asymmetries. Most disproportions in the face are secondary to discrepancies in the middle and inferior thirds.[7]
The ideal candidate for suturing techniques in rhinoplasty has thin skin, strong cartilage, and a wide nasal tip. [8,9] By using suture techniques only, the surgeon can achieve adequate projection and rotation of the nasal tip. These techniques include the dome binding suture, tongue-in-groove procedure, and septocolumelar suture.[10] These techniques have the advantage of preserving nasal tip support mechanisms and present less distortion caused by the wound-healing process.[11] The septocolumelar suture is a loop suture between the medial crura and the caudal septum, and according to the height and direction of penetration into the septum, this suture can increase or decrease the projection and rotation of the nasal tip and increase or decrease the columellar show.[12]
The characteristics of the nasal septum are of special importance in this type of suture technique, so a twisted or weak caudal septum may be a contraindication for this technique unless this portion of the septum is improved surgically before the placement of the suture.[11,13,14] In this article, we describe a consistent method to use this suture technique and place it properly to achieve the best results in the position and shape of the nasal tip.
Description of the Technique
Anesthesia
Under balanced general anesthesia, antisepsis is done with povidone-iodine, placement of surgical fields, infiltration of xylocaine with 1% epinephrine at incision sites, exit sites of nerves, and supratrochlear vessels.
Incision
With a #15 blade, a continuous inter-cartilaginous incision combined with a hemi-transfixion incision is performed bilaterally, and the transfixion is completed. The approach of the tip is done by bilateral marginal incision, performing a bi-pediculated flap, releasing areolar tissue from the dorsal-cephalic border of the alar cartilages.
Management of Lateral Crura
In general, the type of suture used for creating a new dome and managing lateral crura is PDS 5-0, with a few exceptions that are mentioned as follows. To rotate the tip, the surgeon marks a new dome lateral to the original dome. Then, the cephalic edge of the lateral crura is marked, leaving at least 7 mm of lateral crura wide. Then, the surgeon lifts the mucosa from the vestibular face of the cartilage with Iris scissors and makes a partial cut in the cartilage with a No. 15 blade, bending the cephalic border inwards. Then fix the position with two 5-0 PDS horizontal mattress sutures. (Fig 1 A-B)
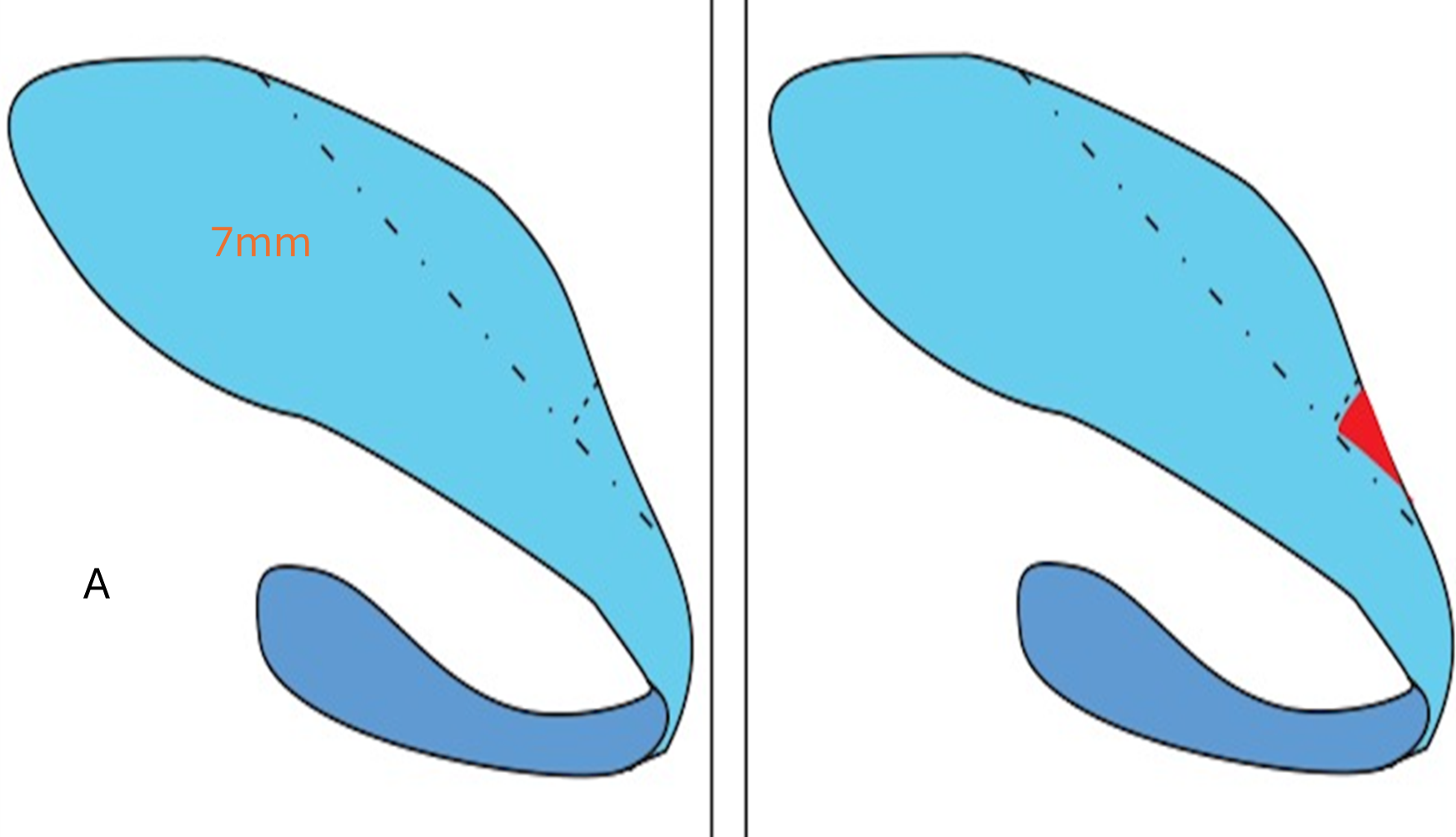
Fig 1. A. Marking of the Lateral Crura at the Level of the New Domes and the Area for the Cephalic Reduction, Leaving At Least 7mm Wide. Resection of the Anterior Portion to Allow the Bending of the Flap.
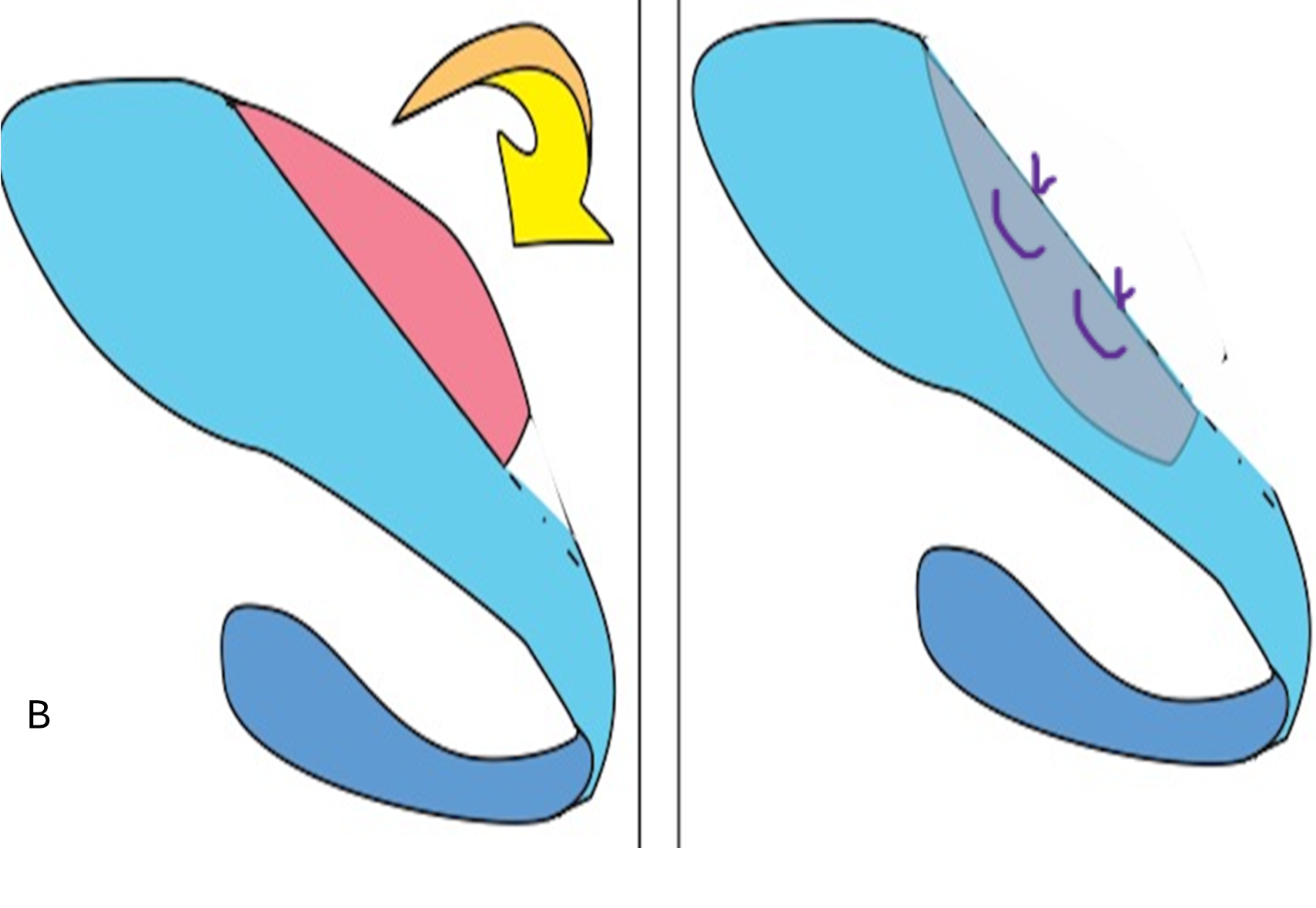
Fig 1. B. Partial Cut of the Cephalic Portion and Bending Over. Fixation with 5-0 PDS Horizontal Mattress Sutures.
Dome Management
A simple stitch is placed in a lateral-to-medial direction through the cephalic-dorsal border of the lateral crura to join it with the cephalic border of the medial crura, approximately 2 mm from the new dome (Gruber suture). This suture allows the domes' cephalic portion to narrow, maintain the caudal portion flare, and achieve more definition of the tip without compromising the internal valve area. A mattress suture is fixed in a medial-to-lateral fashion at the midportion of the new domes, joining the middle and lateral crura (intradomal suture), further improving the definition of the tip.
Septocolumelar Suture
The surgeon then places a Prolene 5-0 suture in the cephalic border of the middle crura, 7mm medial from the new domes, tightening a knot and then fixing this suture 2mm inferiorly to the anterosuperior angle of the caudal septum (ASA). A new Prolene 5–0 stitch is placed 5mm from the domes and fixed in the septum at the ASA level. All these sutures stabilize the nasal tip`s ultimate position by anchoring it to the caudal septum and reducing tilting (Fig. 2A- C).
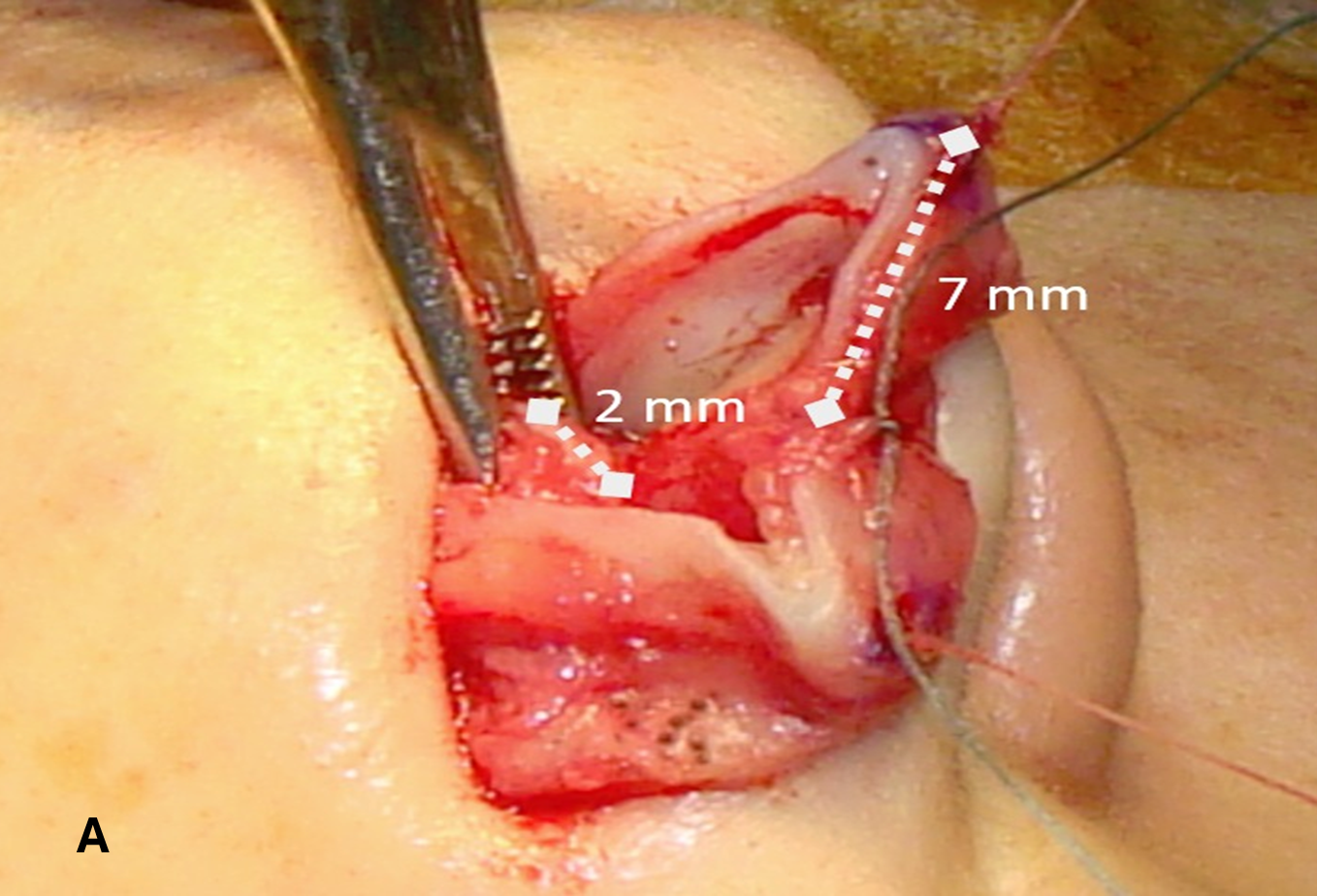
Fig. 2. A. Positioning of Septocolumelar Suture 7mm from the New Domes and 2mm Superior to the Anterosuperior Septal Angle.
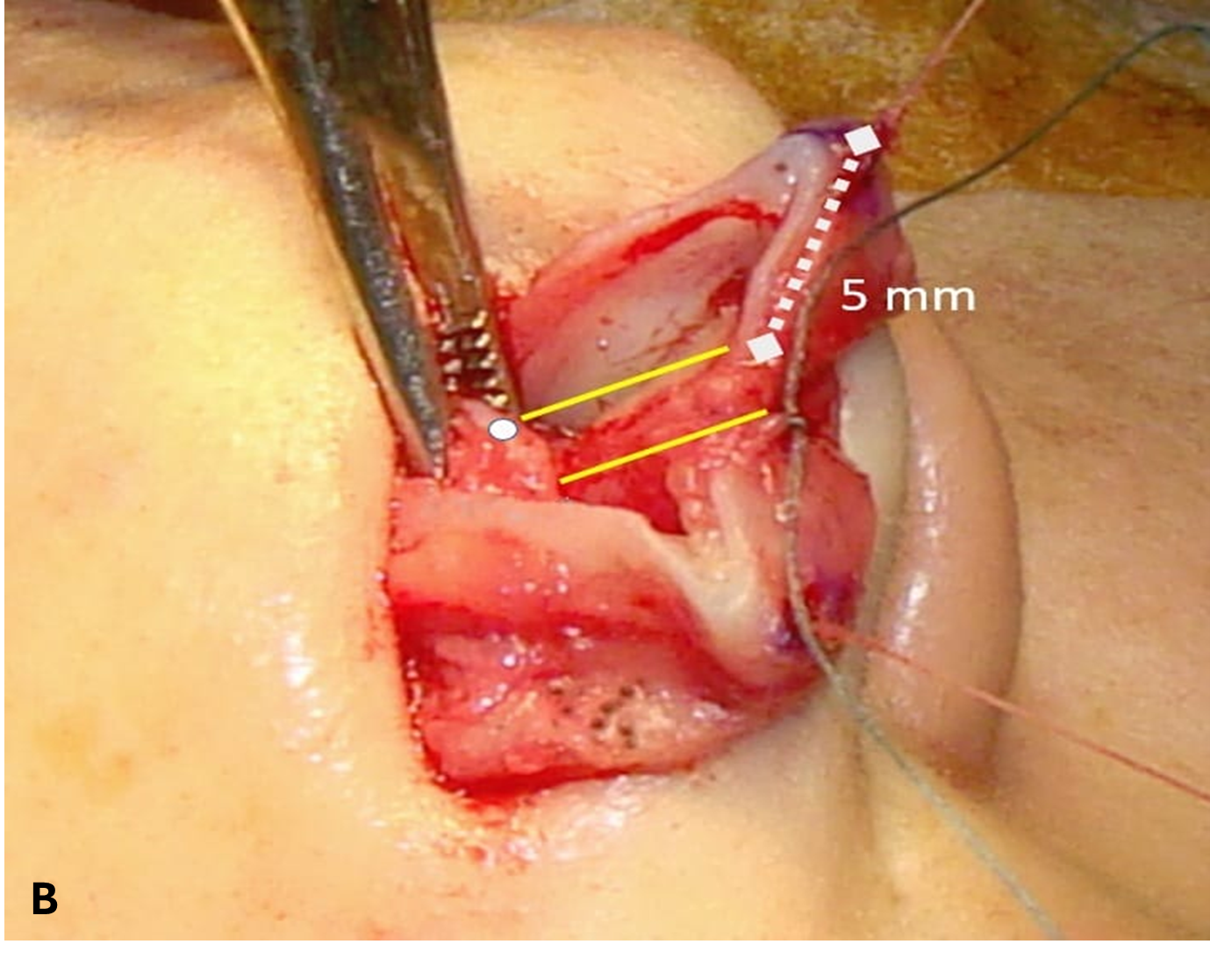
Fig. 2.B. Second Suture Placed at 5 Mm from the New Domes and 2 Mm Caudally in the Septum (Anterosuperior Septal Angle).
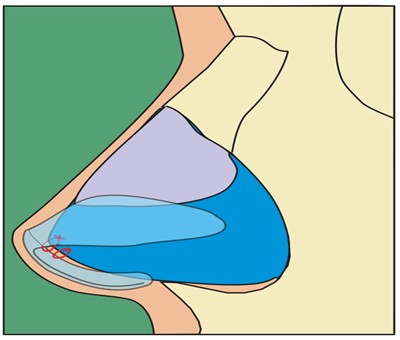
Fig. 2.C. Representation of the Final Position of the Septo-Columelar Sutures.
Modulation of Lateral Crura
In the cephalic portion of the lateral crura of both alar cartilages, a 5-0 PDS "figure-of-8" suture is placed about 5mm from the domes, allowing a more horizontal position of the lateral crura to improve the angle in the scroll area (resting angle) and granting greater permeability to the internal nasal valve. This suture is repeated at 2 mm cephalically to the previous one.
Tip Grafts
Grafts are designed using septal cartilage and placed to give additional support and provide more definition to the nasal tip. We use an intercrural strut graft and a shield-shaped tip onlay graft; both are fixed with 3 simple sutures of PDS 5-0 to the middle crura of the alar cartilages (Fig. 3A and B). Photographic documentation of patients undergoing this combined technique of sutures and grafts for tip management is shown in Figs 4 and 5. (Pictures and release forms added in a separate document).
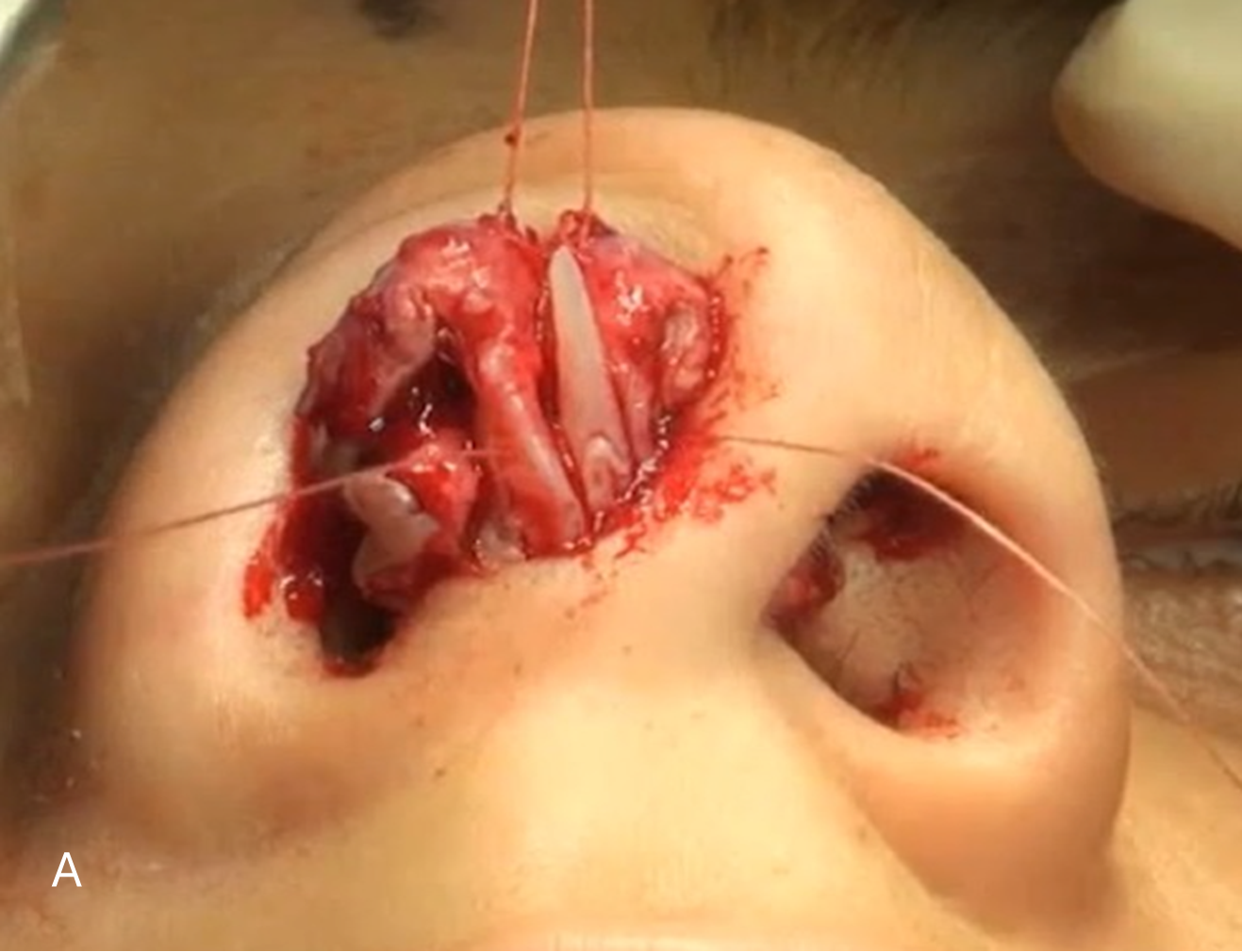
Fig. 3. A. Placement of Intercrural Strut Fixed to the Medial Cruras with 5-0 PDS Simple Sutures.
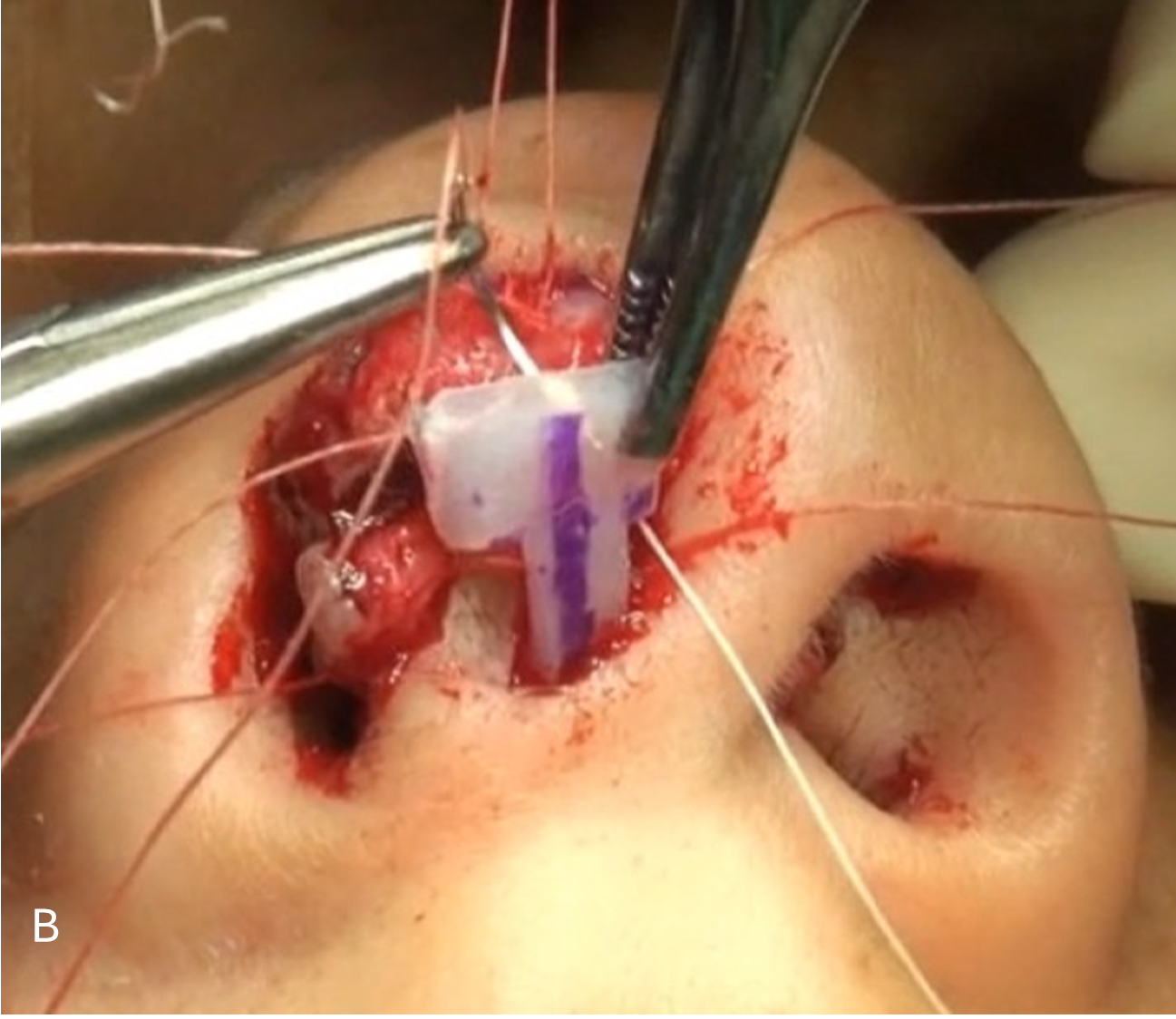
Fig. 3. B. Shield-Shaped Onlay Graft Suture to the New Domes and Medial Cruras with 5-0 PDS.
Fig 4. A, B, C



Fig 5. A, B, C



Discussion
The nasal tip is one of the most challenging areas to manage in plastic surgery. There are different factors to consider during surgery planning; some of these are intrinsic to the alar cartilages, such as shape, definition, and symmetry. Other important factors are the shape and strength of the nasal septum, upper lateral cartilages, and ligament attachments.[11]
There are numerous suture techniques for positioning and reshaping the nasal tip. For the surgeon, it is important not only to dominate the technical aspects of each one of them but also to know the possible indications and side effects.[15] For this instance, some techniques use the cephalic borders of the lower lateral cartilages sutured over the caudal septum, as in the “Hezarfen wings,” to achieve more tip projection with the possible side effect of a visible supratip defect.[16]
One of the most reliable suture techniques for nasal tip management is the septocolumellar suture. Although there are different names for this suture, the principle of the technique is always to place a suture that binds the two middle crura to the caudal septum.[17,18] An important matter about the technique is that in the septo-columellar suture, the surgeon first does the stitch and the knot binding the medial crura and then fixes it to the caudal septum to avoid the cephalic displacement of the medial crura and reduce the risk of columellar retraction. [3,15]
One variation of the septo-columellar suture is the so-called orthopedic suture, which is applied anteriorly in the septum and posteriorly in the columella to increase the projection of the tip. The projection achieved can be combined with cutting the fibers of the depressor muscle of the nasal septum to ensure the permanent stability of the raised tip. A problem with this suture is its placement percutaneously with absorbable sutures or through small mucosal and vestibular skin incisions, sacrificing the proper exposure of the cartilaginous components.[19]
Another type of septocolumelar suture is called "projection control suture." In this one, a Prolene 5/0 penetrates the left medial crura from the outside-in; then the right medial crura from the inside-out; finally, the needle is passed through the septal cartilage at a point that can be anterior, posterior, or at the same level as that performed in the medial crura. The suture is then tied, thus bringing the middle crura to a new position over the nasal septum.[20]
Among all the different techniques, the nasal septum is the most important element to achieve a proper and long-lasting result regarding the position, projection, and rotation of the tip. It becomes necessary to correct any deviations or to improve the thickness of the cartilage if it is too weak. Also, ensuring the septal attachment to the anterior nasal spine is key to stabilizing the whole tip subunit.[21]
Conclusion
The characteristics of the nasal septum, especially the caudal portion, have particular importance for nasal tip suture techniques. The caudal portion of the septal cartilage has a significant influence on the versatility of the septocolumellar suture and the final arrangement of the nasal tip. The septocolumelar suture is a reliable technique that can be used in closed or open rhinoplasty approaches that provide a constant result, giving structure, support, and shape to the ultimate position of the nasal tip.
- ErDem T. (2010). Long-term effectiveness of projection control suture in rhinoplasty. Rhinology. 48(2): 189-194.
- Sciegienka S, Hanick A, Spataro E. (2022). Nasal Tip Support and Management of the Tip Tripod Complex. Clin Plast Surg. 49(1): 61-70.
- Şirinoğlu H. (2017). The Effect of the Short and Floating Columellar Strut Graft and Septocolumellar Suture on Nasal Tip Projection and Rotation in Primary Open Approach Rhinoplasty. Aesthetic Plast Surg. 41(1): 146-152.
- Gruber RP, Weintraub J, Pomerantz J. (2008). Suture Techniques for the Nasal Tip. (Aesthetic Surg J. 28(1): 92-100.
- Perkins S, Patel A. (2009). Endonasal Suture Techniques in Tip Rhinoplasty. Facial Plast Surg Clin North Am. 17(1): 41-54.
- Öztürk G. (2022). Controlling Nasal Tip Projection and Rotation with New Composite Septocolumellar Flap Approaches. Plast Reconstr Surg. 149(4): 669E-678E.
- Sajjadian A, Guyuron B. (2010). Primary rhinoplasty. Aesthet Surg J. 30(4): 527-539.
- Apaydin F. (2016). Projection and Deprojection Techniques in Rhinoplasty. Clin Plast Surg. 43(1): 151-168.
- Tezel E, Ersoy B. (2016). Tip-oriented closed rhinoplasty built on septocolumellar suture and a new caudal septal graft technique. Ann Plast Surg. 77(3): 264-271.
- Pastorek N, Cleveland P. (2022). Improving Projection of the Nasal Tip in Primary Endonasal Rhinoplasty. Facial Plastic Surgery. 38(1): 46-56.
- Lo S, Rowe-Jones J. (2007). Suture techniques in nasal tip sculpture: Current concepts. Journal of Laryngology and Otology. 121(8): 10.
- Bitik O, Uzun H, Kamburoǧlu HO, Dadaci M. (2014). Nasal tip suspending transfixion suture. Aesthetic Plast Surg. 38(2): 309-315.
- Gassner HG. (2010). Structural grafts and suture techniques in functional and aesthetic rhinoplasty manipulation of the cartilaginous skeleton through suture techniques. Current Topics in Otorhinolaryngology - Head and Neck Surgery. 9: 1-19.
- Espinosa-Reyes JA, Solis-Ruiz LA. (2020). Overprojected Nasal Tip: Technique To Decrease The Nasal Tip Projection. Rhinoplasty Archive.
- Lo S, Rowe-Jones J. (2007). Suture techniques in nasal tip sculpture: Current concepts. Journal of Laryngology and Otology. 121(8): 10.
- Yeşiloǧlu N, Sarici M, Temiz G, Yildiz K, Mersa B, Filinte GT. (2014). Hezarfen wings: A lower lateral cartilage-based cartilage suspension technique for the adjustment of nasal tip rotation and projection and the correction of supratip deformity. Journal of Craniofacial Surgery. 25(3): 983-987.
- Tezel E, Numanoǧlu A. (2007). Septocolumellar suture in closed rhinoplasty. Ann Plast Surg. 59(3): 268-272.
- Demirbilek N, Evren C, Elbistanlı MS, Altun U, Günay SS. (2016). Técnica de sutura septocolumelar em dois níveis para correção de desvio septal caudal. Braz J Otorhinolaryngol. 82(4): 403-407.
- Gustave B. Fred. (1958). Evaluation of the orthopedic septocolumellar suture in rhinoplasty. The Laringoscope. Published online. 1700-1705.
- Daley J. (1945). ROLE OF COLUMELLAR AND SEPTOCOLUMELLAR SUTURES IN RHINOPLASTY. Arch Otolaryng. 42(33): 178-190.
- Akkus AM, Eryilmaz E, Guneren E. (2013). Comparison of the effects of columellar strut and septal extension grafts for tip support in rhinoplasty. Aesthetic Plast Surg. 37(4): 666-673.
Download Provisional PDF Here
PDF