

p (1).png)



.png)




.png)

Case Report
Casuistic Case of Iatrogenic Foreign Bodies Migration
- Sivakon Stanislav Vladimirovich
Corresponding author: Sivakon Stanislav Vladimirovich, Doctor of Medical Sciences, Head of the Department of Traumatology, Orthopedics and Military-Extreme Medicine of Penza State University, Russia, Penza, Krasnaya Street, 40, phone: +7(961)352-89-18.
Volume: 3
Issue: 2
Article Information
Article Type : Case Report
Citation : Sivakon Stanislav Vladimirovich. Casuistic Case of Iatrogenic Foreign Bodies Migration. Journal of Medical and Clinical Case Reports 3(2). https://doi.org/10.61615/JMCCR/2026/APRIL027140429
Copyright: © 2026 Sivakon Stanislav Vladimirovich. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.61615/JMCCR/2026/APRIL027140429
Publication History
Received Date
10 Apr ,2026
Accepted Date
23 Apr ,2026
Published Date
29 Apr ,2026
Abstract
The article describes two casuistic cases of Kirschner wire migration during osteosynthesis of the acromioclavicular joint. In both cases, the fragments of the wires migrated towards the spine and entered the spinal canal.
Keywords: foreign body migration; Kirschner wire; osteosynthesis of the acromioclavicular joint.
►Casuistic Case of Iatrogenic Foreign Bodies Migration
Sivakon Stanislav Vladimirovich1*
1Doctor of Medical Sciences, Head of the Department of Traumatology, Orthopedics and Military-Extreme Medicine of Penza State University, Russia, Penza, Krasnaya Street, 40.
Introduction
One of the complications of osteosynthesis is the migration of metal structures. Kirschner wires are the most commonly migrated due to their streamlined shape and small cross-section. Migration of wires occurs after the end of immobilization and the restoration of active movements. Typically, a migrating wire shifts within the same limb segment and protrudes under the skin, sometimes perforating it.
In 2011, a 32-year-old patient B. came to the clinic with complaints of pain in the coccyx area. An X-ray examination revealed a foreign body in the patient's lumbar-sacral spine region, a 6-cm-long fragment of a Kirschner wire. (Fig. 1).
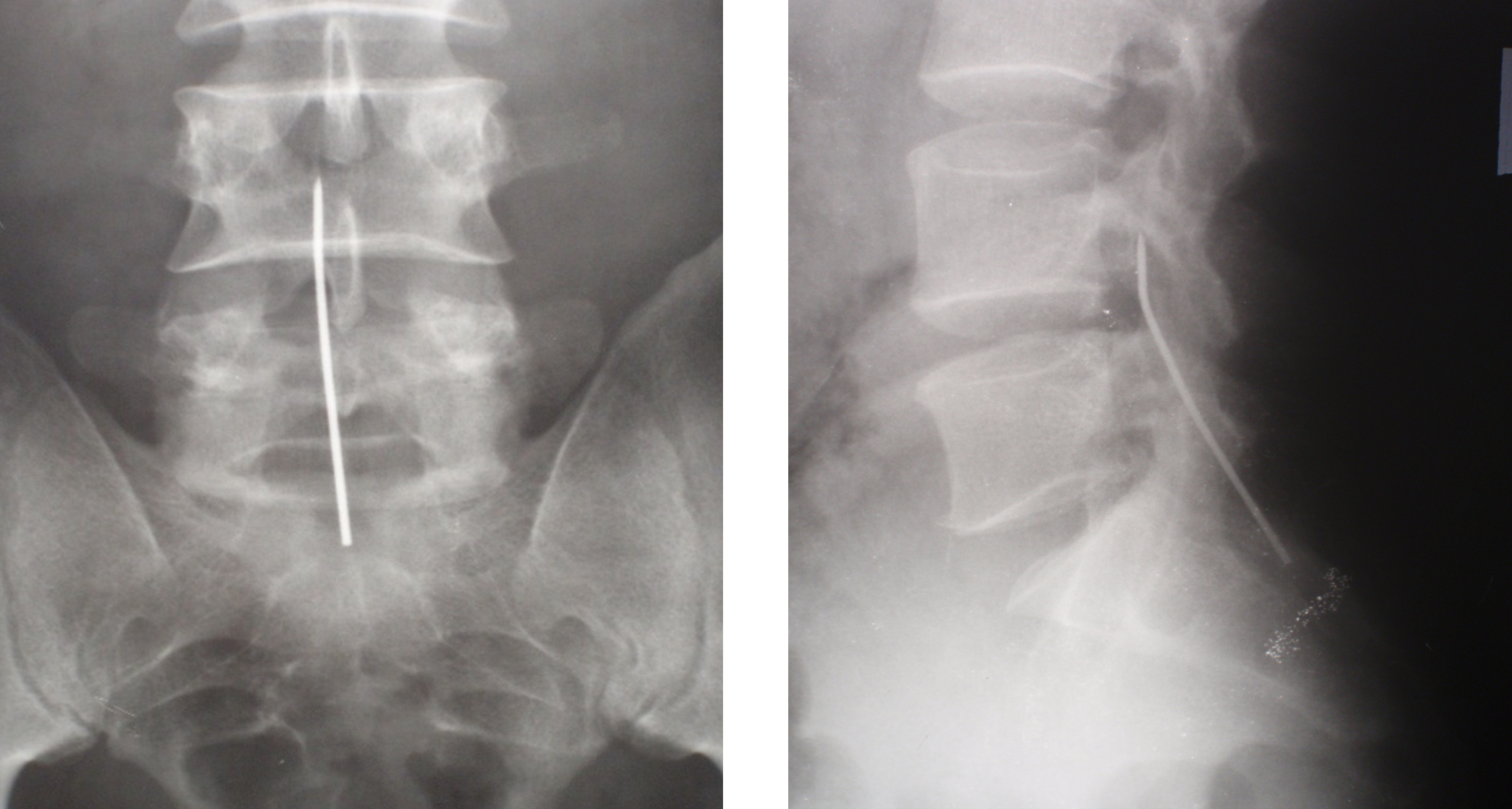
Figure 1. X-ray images of the lumbar-sacral spine of patient B. The foreign body is a fragment of a Kirschner wire
From the anamnesis, it was found out that in 1999, the patient was operated on in another clinic for damage to the acromioclavicular joint on the right. Osteosynthesis was performed with two crossed Ktrshner wires. After 4 weeks, postoperative immobilization was stopped, and the patient was discharged to work, but the wires were not removed. In 2009, the patient experienced pain in the neck for several months. The neurologist prescribed treatment, including massage, and the pain gradually subsided.
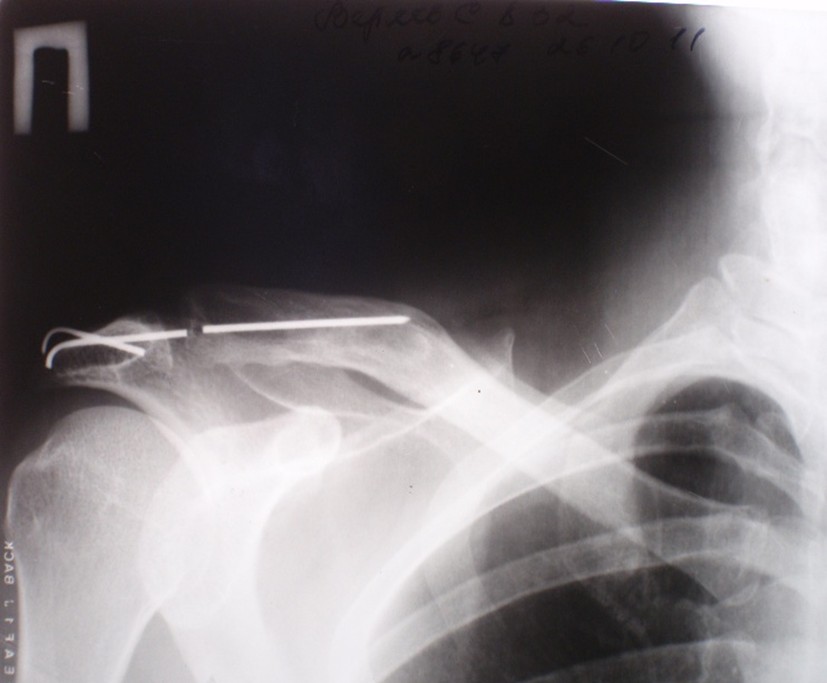
Figure 2. X-ray of the right shoulder joint of patient B. Fracture of the spokes and absence of one of the proximal fragments.
In order to clarify the localization of the broken-off wire, a magnetic resonance imaging of the lumbosacral spine was performed, which revealed the location of the wire in the lumen of the spinal canal. In addition, there was a destruction of the lower part of the sacrum and a tumor-like formation extending towards the rectum (Fig. 3). As a result of a consultation with neurosurgeons and oncologists, it was determined that the pain syndrome was caused by the presence of a tumor, and the patient was not bothered by the wire. The patient was referred to an oncology clinic.
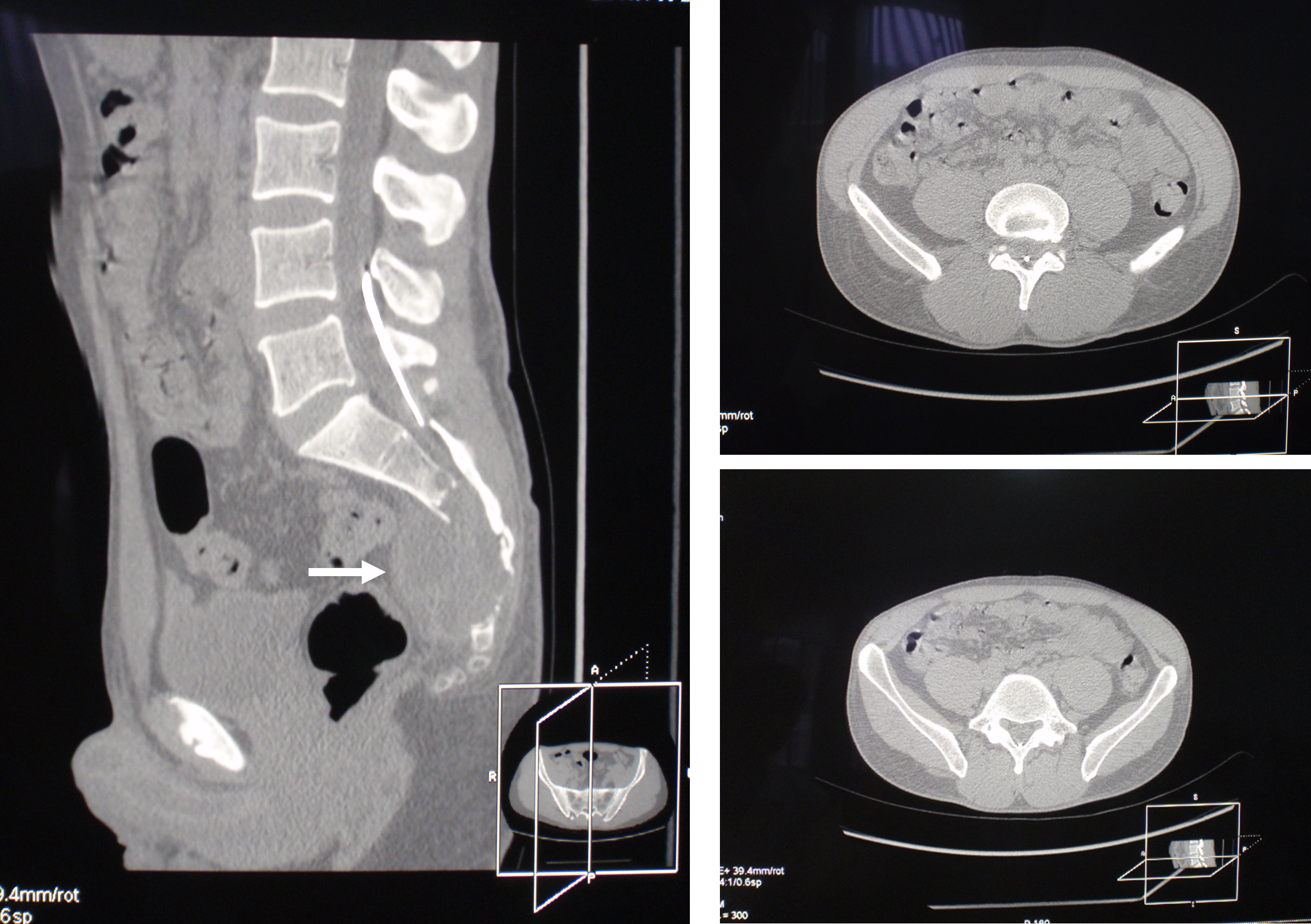
Figure 3. MRI of the lumbosacral spine of patient B. The foreign body is located in the spinal canal at the level of L4, L5, and S1 vertebrae. The arrow indicates a tumor-like formation and a zone of sacral destruction.
Discussing the migration path of the needle, we assumed that initially one of the needles was located outside the clavicle, along its lower edge. After the beginning of active movements in the shoulder girdle, the needles broke. One of them, located in the clavicle, remained in place, and the other appeared in the fascial space between the chest and the muscles surrounding the shoulder blade. The movement of the shoulder gradually shifted the needle towards the spine with a sharp end forward. Later, apparently in 2009, the wire was inserted between the vertebrae and turned with its sharp end pointing upwards towards the brain (the radiograph shows that the sharp end of the wire is slightly curved 1.5 to 2 cm from the sharp end). Movements in the cervical spine displaced the needle upward until it was completely in the spinal canal, after which it began to "fall" downwards with the blunt end forward. It is amazing that the needle did not damage the spinal cord or the roots of the spinal nerves during its migration. Given the extent of damage to the posterior regions of the L4, L5, and S1 vertebrae, which was necessary to remove the foreign body, and the absence of any symptoms, surgical treatment was deemed unnecessary.
The correctness of our assumptions was confirmed when, after some time, a 40-year-old patient C came to the clinic with complaints of pain in the cervical spine. In 2007, he underwent osteosynthesis of the acromioclavicular joint with two crossed Kirschner wires, which were also not removed. An X-ray examination revealed a fracture of the wires, migration of one of the fragments, and its insertion into the cervical spine (Fig. 4). The patient underwent surgery, and the foreign bodies were removed.
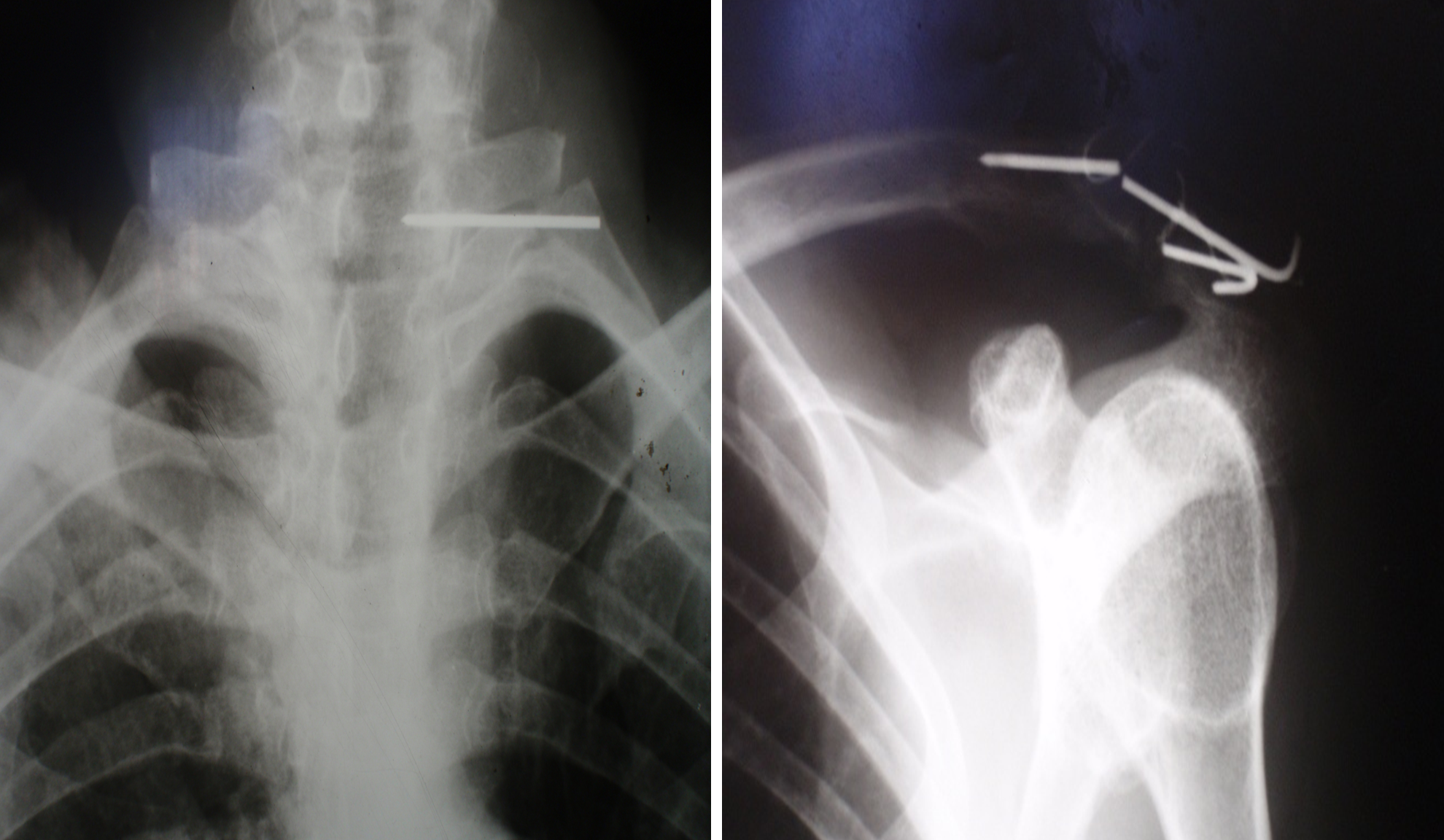
Figure 4. X-ray images of the left shoulder joint and the cervical spine of patient C. Fracture of the pins and migration of one of the proximal fragments.
Сonclusion
In summary, it is important for practicing orthopedic traumatologists to remove Kirschner wires before starting rehabilitation procedures and restoring active limb movements.
- Lee JH, Chung JY, Kim MS. (2014) Unusual migration of Kirschner’s wire into intervertebral foramen after lateral clavicle fracture fixation – a case report. Clin Shoulder Elbow. 17(2):77-79.
- Mankowski B, Polchlopek T, Strojny M, Grala P, Slowinski K. (2016). Intraspinal migration of a Kirschner wire as a late complication of acromioclavicular joint repair: a case report. J Med Case Rep. 10:66.
- Gonsales D, Aguilar-Salinas P, Cavicchioli A, (2017) The Migration of Kirschner Wire from Left Distal Clavicle to the Intradural Anterior Thoracic Spine. Open Access J Neurol Neurosurg. 2(4).
Download Provisional PDF Here
PDF