

p (1).png)



.png)




.png)

Case Study
Advanced Anesthesia Circuit Management in Facial Plastic Surgery: Enhancing Safety and Efficiency
- Jorge Alberto Espinosa-Reyes
Corresponding author: Jorge Alberto Espinosa-Reyes, MD, ENT, Facial Plastic Surgeon Calle 127a # 7- 53 cons 3005 (INO), Bogotá, Colombia, ORCID: 0009-0008-7673-586x
Volume: 3
Issue: 1
Article Information
Article Type : Case Study
Citation : Jorge Espinosa, Juan Ochoa, Freddy Rodriguez, Ana Milena Garcia, Roberto Quijano, Laura Camila Botero Díaz. Advanced Anesthesia Circuit Management in Facial Plastic Surgery: Enhancing Safety and Efficiency. Journal of Medical and Clinical Case Reports 3(1). https://doi.org/10.61615/JMCCR/2026/MAR027140304
Copyright: © 2026 Jorge Alberto Espinosa-Reyes, MD. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.61615/JMCCR/2026/MAR027140304
Publication History
Received Date
05 Feb ,2026
Accepted Date
16 Feb ,2026
Published Date
04 Mar ,2026
Abstract
Background: Facial plastic surgery frequently necessitates the use of general anesthesia, with the breathing circuit positioned within a confined surgical field. The proximity of the circuit to the operative area, coupled with the surgeon's manipulations, heightens the risk of endotracheal tube displacement and circuit disconnection, potentially resulting in severe hypoxia or airway disruption. Consequently, the anesthesiologist must implement additional measures to secure the tube using tapes or sutures. However, the surgeon must also maintain the sterility of the field, which often requires covering the tube or circuit with sterile sheets, thereby obstructing the anesthetist's visual field control. Although advancements in ventilatory monitoring have been made, visual confirmation of circuit integrity remains essential yet is frequently overlooked. The current literature lacks comprehensive guidance on sterile circuit management strategies specific to facial plastic surgery.
Objective: This study elucidates an advanced methodology for integrating a sterile anesthesia circuit to facilitate continuous visual monitoring during facial plastic surgery. This approach aims to mitigate the risk of disconnection while maintaining sterility and operational efficiency. The study establishes the technique's feasibility and safety within a high-volume cohort. Enhanced visibility and stabilization of the anesthesia circuit can significantly reduce life-threatening airway complications. By ensuring continuous visualization of the tube for both the surgeon and anesthesiologist, this technique enhances perioperative safety and patient outcomes in procedures with a high risk of airway compromise. Given that this study is situated within the context of facial plastic surgery, nearly all procedures involving the face, head, neck, and oral and nasal cavities necessitate reliable airway protection strategies, which are essential for ensuring patient safety.
Keywords: Anesthesia circuit management, Endotracheal tube stabilisation, Airway safety, Intraoperative airway monitoring, Circuit disconnection prevention
Graphical Abstract

►Advanced Anesthesia Circuit Management in Facial Plastic Surgery: Enhancing Safety and Efficiency
Jorge Espinosa MD1*, Juan Ochoa MD2, Freddy Rodriguez MD3, Ana Milena Garcia MD4, Roberto Quijano MD5, Laura Camila Botero Díaz6
1ENT and Surgery Fellowship professor – The Face & Nose Institute, Universidad Militar, Universidad Javeriana de Cáli, Calle 127a # 7- 53 cons 3005 (INO), Bogotá, Colombia, ORCID: 0009-0008-7673-586x.
2ENT, Facial Plastic Surgeon. Bogotá, Colombia, ORCID: 0009-0003-5224-0663.
3Department of Anesthesiology, Calle 127a # 7- 53 (INO), Bogotá, Colombia, ORCID: 0009-0001-1470-1735.
4Department of Anesthesiology, Calle 127a # 7- 53 (INO), Bogotá, Colombia, ORCID: 0009-0004-1169-1238.
5ENT and Facial Plastic Surgery Fellow – The Face & Nose Institute, Bogotá 110121, Colombia, ORCID: 0009-0005-6337-8347.
6Fourth-Year Otolaryngology Resident, Department of Otolaryngology–Head and Neck Surgery, Universidad Militar Nueva Granada / Hospital Militar Central, Bogotá, Colombia.
Introduction
According to the International Society of Aesthetic Plastic Surgery (ISAPS), the total number of procedures performed in 2024 included 737,028 facelifts (4.2%), 524,386 browlifts (3%), and 477,624 necklifts (2.7%). These statistics indicate that facial plastic surgery encompasses a diverse range of procedures, from aesthetic enhancements to reconstructive interventions, often necessitating general anesthesia to ensure both patient comfort and surgical precision. The anesthesia circuit, an essential component of the anesthesia delivery system, is crucial in maintaining adequate oxygenation, ventilation, and anesthetic gas delivery [1]. Accidental disconnection of components of the breathing system during general anesthesia with an endotracheal tube remains an occasional issue, particularly in facial surgery, where the tube is situated within an active surgical field and is not readily accessible to the anesthesiologist [1-2].
Even if modern monitoring will always sound the alarms in case of disconnection, the anesthesiologist's stress and the change of potential danger are still issues to talk about and improve.
The challenges in anesthesia circuit management in facial plastic surgery include the sharing of the field with the surgeon's team, restricted access to the airway, potential airway compromise, and the need for precise ventilation to avoid hypoxia or hypercapnia. [1-2]
The significance of advanced anesthesia circuit management lies in its direct impact on patient safety and surgical efficiency. Effective management minimises the risk of complications associated with general anesthesia, such as respiratory depression, airway obstruction, and anesthetic gas leaks, which can lead to adverse outcomes.
Furthermore, optimizing the anesthesia circuit design and operation enhances surgical workflow, reduces operative time, and improves recovery outcomes. [1-2] As facial plastic surgery continues to evolve with advancements in techniques and technology, the need for specialized anesthesia circuit management strategies has become increasingly critical. [1-2]
We aimed to demonstrate the successful execution of all facial plastic surgery procedures, which inherently present a high risk of airway disconnection or related complications, performed safely by a single surgeon without resulting in any morbidity or mortality.
Institutional Setting
The INO Ophthalmic and Plastic Surgery Institute (INO), located in Bogotá, Colombia (Calle 127A # 7-53), functioned as the central hub for all facial plastic and reconstructive surgeries performed by Dr. Jorge Alberto Espinosa Reyes from 2023 to 2025. INO is a modern, purposefully designed facility comprising six operating rooms according to high international standards.
Design
A retrospective review was conducted on all patients undergoing cervicoplasty and rhytidoplasty by Dr Jorge Espinosa at the INO Ophthalmic and Facial Plastic Surgery Institute (INO) in Bogotá, Colombia, between January 1, 2023, and December 31, 2025. INO is a high-volume tertiary care center dedicated to facial plastic and reconstructive surgery, equipped with six operating rooms, a dedicated outpatient clinic, and state-of-the-art anesthetic infrastructure.
Anesthetic Circuit Integration Technique
Cosmetic surgery encompasses an expanded spectrum of procedures that vary greatly in complexity, duration, and complications. They range from “simple” surgeries such as scar correction, mentoplasty procedure “complex” surgeries such as ritidoplasty, cervicoplasty, blepharoplasty, and nose surgery.
Following the completion of the difficult airway risk stratification and the resolution of all relevant pre-intubation anamnesis, the procedure commenced with fixation of the endotracheal tube at the upper labial frenulum using 2–0 silk, securing it to the central portion of the tube selected based on each patient’s airway characteristics. Subsequently, standard aseptic and antiseptic surgical protocols were initiated. With the assistance of an additional team member, the endotracheal tube, filter, and the initial anesthetic breathing circuit were elevated (Fig. 1). Once elevated, the routine sterile draping sequence was performed without contaminating any component (Fig 1). The Gillies drape was applied, followed by two short drapes over the thoracic region, and finally a sterile surgical sheet. After draping, the anesthetic circuit was exchanged in a sterile manner (Fig 2). This technique ensures that the connection to the endotracheal tube remains straightforward, transparent, visible, and securely fixed, allowing continuous visual control by both the anesthesiologist and surgeon, while maintaining a fully sterile operative field (Fig 3).
Video 1. Advance Anesthesia Circuit Management in FPS
https://www.kapwing.com/videos/699576c6d85dad76fc2b47dc
Fig 1. Sterile Placement Technique of the Anesthetic Breathing Circuit
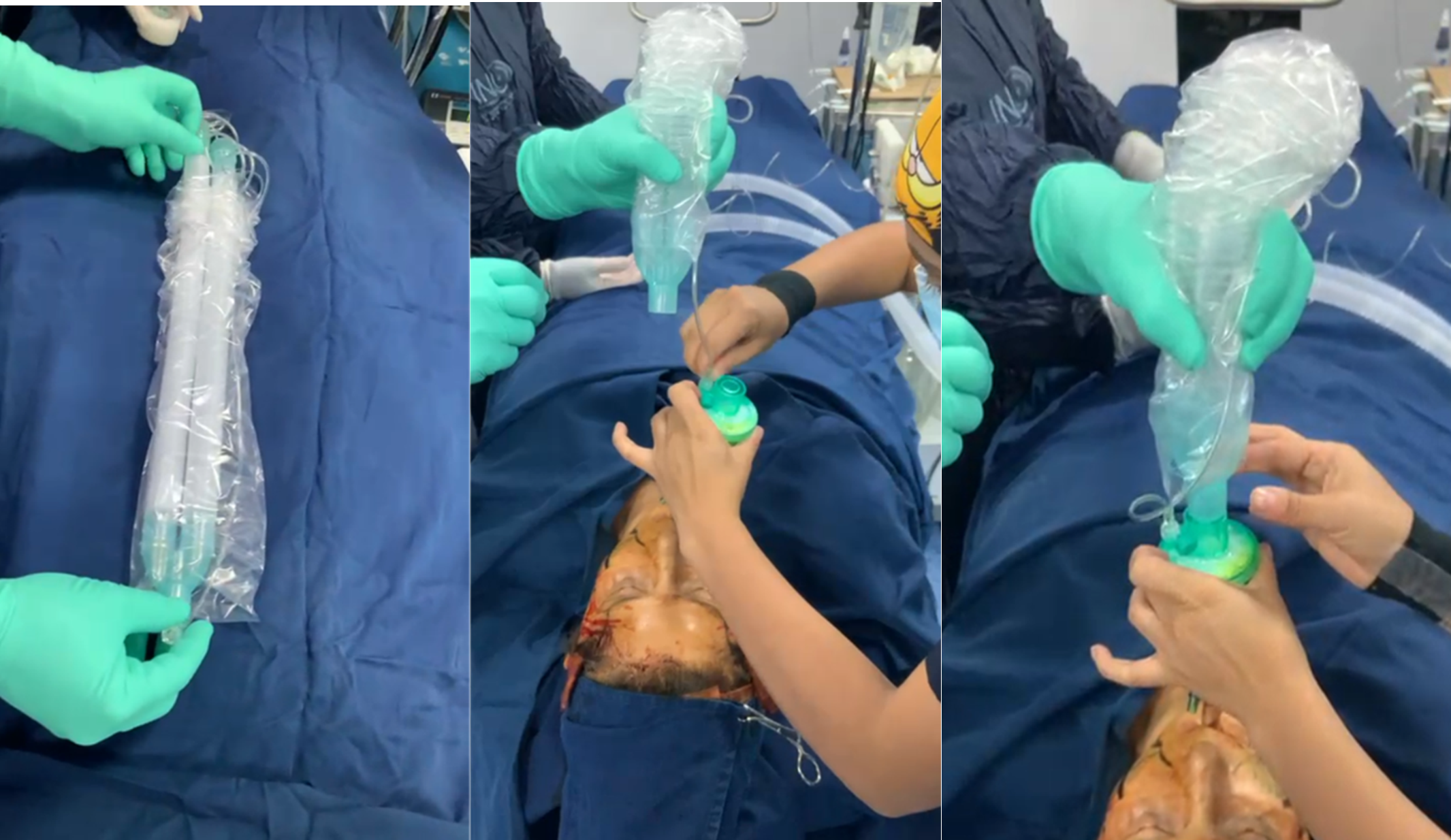
a. Preparation of the sterile anesthetic circuit.
b. Placement of the sterile segment of the anesthetic circuit onto the non-sterile filter attached to the endotracheal tube (held by a non-sterile assistant).
c. Advancement of the sterile circuit sleeve over the filter and endotracheal tube.
Fig 2. Progression and Final Outcome of the Sterile Anesthetic Circuit Exchange

a. Cranial fixation using a minimal amount of adhesive tape to maintain transparency and allow visualization of the endotracheal tube.
b. Caudal fixation of the circuit.
c. Final placement of the anesthetic circuit in a fully sterile manner.
Fig 3: Optimal Final Placement of the Endotracheal Tube Ensuring Full Visibility and Airway Safety.

Results
The cohort comprised 160 consecutive patients treated by Dr. Espinosa during the study period, consisting of 140 female and 20 male patients. Of these, 50 cases underwent cervicoplasty, while 110 underwent rhytidoplasty. The inclusion criteria specified patients aged ≥ 18 years who underwent primary elective surgery performed by Dr. Espinosa within the defined timeframe. Patients with incomplete medical records or follow-up of less than 3 months were excluded. Notably, no patient experienced any anesthetic complications or episodes of endotracheal tube disconnection throughout the perioperative period. (Tab 1)
Table 1. Demographic and Clinical Characteristics of the Study Cohort (2023–2025)
|
Characteristic |
n (%) |
Details |
|
Total Patients |
160 (100%) |
Consecutive cases during the study period |
|
Sex |
||
|
• Female |
140 (87.5%) |
|
|
• Male |
20 (12.5%) |
|
|
Age |
— |
Adults ≥18 years (mean age 55 years) |
|
Procedure Type |
||
|
• Rhytidoplasty |
110 (68.8%) |
Primary elective cases |
|
• Cervicoplasty |
50 (31.2%) |
Primary elective cases |
|
Exclusion Criteria |
— |
Incomplete medical records or <3 months follow-up |
|
Safety Outcomes |
0 (0%) |
No anesthetic complications; no endotracheal tube disconnections |
Limitations and Drawbacks
While the advanced anesthesia circuit management detailed in this article offers significant improvements in safety and monitoring, it also presents notable drawbacks that require careful consideration. The implementation of an enhanced anesthetic circuit, which includes the placement of filters, additional checks of non-return valves, inspection of disposable tubing, and integrity testing, may extend the induction and setup period, thereby increasing the total time required for surgery. This additional duration, when accumulated across multiple cases, can diminish overall operating room efficiency and limit patient throughput in high-volume surgical units. Moreover, the use of extra consumables, such as specialized filters and potentially higher-quality or dedicated circuits, along with the additional manpower and training necessary for proper application, may substantially increase per-case costs. Such increased costs could pose a barrier to adoption, particularly in resource-limited settings.
Discussion
Disconnection of the anesthesia breathing circuit during surgical procedures can result in immediate and potentially life-threatening complications, such as hypoxia and hypoventilation, necessitating prompt detection and rectification.
An anesthesiologist can identify this issue by the anesthesia device alarm, recognizing the audible hissing sound or collapse of the breathing bag, as well as by observing a decrease in oxygen saturation or tidal volume.
To address this emergency, anesthesiologists should switch [1] to manual ventilation using a bag-valve mask and give IV anesthetics until circuit reconnection.[4]
Recent literature advocating the use of supraglottic airway devices predominantly supports the adoption of new-generation models. [5] These advanced devices are constructed with thermosensitive materials that adapt to the patient's anatomical structure through body heat, thereby enhancing sealing efficacy while reducing mucosal trauma [5].
In contrast, earlier generation supraglottic devices, although more cost-effective, are susceptible to displacement, improper positioning, leakage, and diminished stability [5]. Such leakage is particularly problematic in the context of facial plastic surgery, in which the escape of oxygen into the surgical field significantly increases the risk of fire and other catastrophic events. Furthermore, the propensity of older devices to shift or become dislodged presents additional risks, including loss of airway control [6].
Facial, nasal, and oral procedures also involve blood and secretions, which further increase the likelihood of laryngospasm aspiration during surgery [5-6]. Consequently, anesthesiologists generally prefer to maintain the airway with an endotracheal tube, especially during procedures that may require changes in the patient´s head position or manipulation of the breathing circuit by the surgical team.
Although facial surgeries are often of relatively short duration, positional changes and frequent adjustments in the operative field render supraglottic devices more prone to dislodgement [7]. Notably, the supraglottic devices endorsed in the current literature pertain to specific new-generation models.
As these advanced devices are not yet available in our setting, their advantages cannot be extrapolated to older supraglottic devices in routine use [4]. Therefore, it is advisable to ascertain whether the referenced article pertains to one of these newer models; if so, we can review it together to ensure accurate interpretation within the context of our practice.
Proficiency in circuit design and gas management is essential for the safe administration of anesthesia. Numerous case reports have underscored the significance of recognizing disconnections, leaks, and obstructions within breathing circuits [9-10-11-12]. Team errors are common in airway management [13-14]. A retrospective study investigating the influence of human error in this domain revealed that human mistakes were responsible for 82% of adverse patient outcomes, while equipment malfunctions accounted for only 14% of cases [15]. All case reports concluded that direct visualization of the oxygen circuit could have prevented the desaturation observed in all instances. Therefore, it is imperative to inform every surgeon practicing either cosmetic or reconstructive facial plastic surgery of this alternative and secure method for monitoring the anesthetic circuit.
The complication most frequently encountered during endotracheal tube manipulation is potentially fatal. Medical literature documents instances of severe cerebral hypoxia, respiratory acidosis, and even mortality resulting from unintended disconnection of the endotracheal tube. This risk is further heightened in operating rooms with loud background music or when alarm volumes are inadequately set, underscoring the necessity for both the surgeon and anesthesiologist to maintain continuous oversight of the tube. An alternative method to secure the breathing circuit over sterile drapes, while preserving sterility nd ensuring partial visibility to both the anesthesiologist and surgeon, is sterile bandaging (Fig 5). Although this can be a useful option, it is not entirely reliable; if a disconnection occurs, visualization through the bandage may be insufficient, hindering prompt detection. Therefore, it cannot be considered a fully dependable solution [1].
Fig 4: Illustration of the hazards Associated with Wrapping the Anesthesia Breathing Circuit, Which Prevents Timely Visual Detection of an Accidental Endotracheal Tube Disconnection.
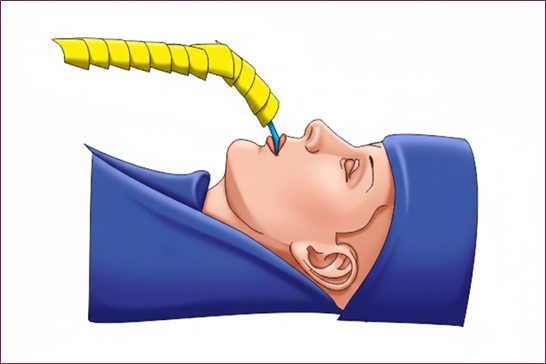
Fig 5: Proper Placement of an Endotracheal Tube (ETT) Within the Airway Position Appropriate for Surgical and Anesthetic Use.

Conclusion
Advanced anesthesia circuit management is the cornerstone of safe and efficient facial plastic surgery, with significant implications for patient outcomes and surgical success. Current research has made notable strides in airway management, circuit design, and complication prevention; however, challenges remain in terms of accessibility, compatibility, and training. Future advancements in technology and interdisciplinary collaboration hold promise for overcoming these barriers and revolutionizing anesthesia circuit management in this specialized field. As facial plastic surgery continues to advance, the development of tailored anesthesia circuit solutions is critical for enhancing patient safety and optimizing surgical outcomes.
This literature review underscores the importance of continued innovation and research in anesthesia circuit management for facial plastic surgery, highlighting its potential to transform surgical practice and improve patient care.
Acknowledgment
The authors would like to express their gratitude to the surgical and nursing teams at the Instituto Nacional de Oftalmología (INO) in Bogotá, Colombia, for their invaluable support during patient care and postoperative follow-up. Special thanks to the Department of Otolaryngology and Facial Plastic & Reconstructive Surgery and Anesthesiology for providing the clinical setting and academic environment that made this work possible. The authors also acknowledge the patients for their trust in and consent to share their clinical cases for educational and scientific purposes.
Conflicts of Interest: None declared
Declarations
Funding: None
Conflicts of Interest: None declared
Ethical Approval: Not required
Patient Consent
Written informed consent was obtained from all the patients for the use of clinical photographs.
- Cullen, D. J, Eichhorn, J. (2007). Wrap Delays Detection of Disconnect. The Official Journal Of The Anesthesia Patient Safety Foundation. 22(2): 25-40.
- Nath, S. S, Roy, D, Ansari, F, Pawar, S. T. (2013). Anaesthetic complications in plastic surgery. Indian Journal Of Plastic Surgery. 46(2): 445-452.
- Khan, M. J, Tageldin, T, Farooqi, M. W, Khamash, O. Q, Shahid, U, Abdul-Rahman, M. E, Elarref, M, Hassan, J. (2020). Principles of Anesthesia and Airway Management in Head and Neck Surgery. En IntechOpen eBooks.
- Hagberg, C. A. (2019). Combined fellowship training in head and neck anesthesia and advanced airway management. Journal Of Head & Neck Anesthesia. 3(1): 9.
- Nair, A, Borkar, N, Murke, S. S, Dudhedia, U. (2024). Safety and Efficacy of the Use of Supraglottic Airway Devices in Children and Adolescents Undergoing Adenotonsillectomy—A Systematic Review and Meta-Analysis. Journal Of Personalized Medicine. 14(3): 311.
- Thomsen, J. L. D, Nørskov, A. K, Rosenstock, C. V. (2018). Supraglottic airway devices in difficult airway management: a retrospective cohort study of 658,104 general anaesthetics registered in the Danish Anaesthesia Database. Anaesthesia. 74(2): 151-157.
- Cook, T, Howes, B. (2010). Supraglottic airway devices: recent ad vances. Continuing Education In Anaesthesia Critical Care & Pain. 11(2): 56-61.
- Walker, S. G, Packiasabapathy, S, Sheplock, G, Acquaviva, M. A. (2021). Breathing circuits. En Elsevier eBooks. 100-124.
- Nandwana, D, Singh, S, Singh, G. P, Ravi, S. (2023). Breathing circuit leak – an unexpected finding. Korean Journal Of Anesthesiology. 76(6): 640-641.
- Dain, S. (2001). Breathing circuit disconnections: averting catastrophes. Canadian Journal Of Anesthesia/Journal Canadien D Anesthésie. 48(9): 840-843.
- Shetty, S. V, Shetty, V. L, Baria, G. D, Sawant, N. G, Sawant, N. G. (2021). Modifications in anesthesia techniques and safety protocols at the outset of the COVID-19 pandemic, in a tertiary care center. Journal Of Clinical Surgery And Research. 2(2): 01-06.
- Apfelbaum, J. L, Hagberg, C. A, Connis, R. T, Abdelmalak, B. B, Agarkar, M, Dutton, R. P, Fiadjoe, J. E, Greif, R, Klock, P. A, Mercier, D, Myatra, S. N, O’Sullivan, E. P, Rosenblatt, W. H, Sorbello, M, Tung, A. (2021). 2022 American Society of Anesthesiologists Practice Guidelines for Management of the Difficult Airway. Anesthesiology. 136(1): 31-81.
- Simpson, J. (2005). Rapid sequence intubation in the emergency department: 5 year trends. Emergency Medicine Journal. 23(1): 54-56.
- Kapadia, F. N, Bajan, K. B, Raje, K. V. (2000). Airway accidents in intubated intensive care unit patients: An epidemiological study. Critical Care Medicine. 28(3): 659-664.
- Cooper, J. B, Newbower, R. S, Long, C. D, McPeek, B. (1978). Preventable anesthesia mishaps. Anesthesiology. 49(6): 399-406.
Download Provisional PDF Here
PDF