

p (1).png)



.png)




.png)

Research Article
Results of Surgical Treatment of Complicated Forms of Autoimmune Thyroiditis
- Fatta Gafar Oglu Sadikhov
Corresponding author: Fatta Gafar Oglu Sadikhov, Candidate of medical sciences, researcher at the department of endocrine surgery of the Scientific Center of Surgery named after M.A. Topchubashov, surgeon-endocrinologist. Address: Republic of Azerbaijan, Baku. AZ 1116, Binagadi district, Baku-Gars 143 st., floor 6, ap. 5. Tel: +994 50 372 50 77, ORCID: https://orcid.org/0000-0002-6779-8796
Volume: 3
Issue: 1
Article Information
Article Type : Research Article
Citation : Fatta Gafar Oglu Sadikhov. Results of Surgical Treatment of Complicated Forms of Autoimmune Thyroiditis. Journal of Medical and Clinical Case Reports 3(1). https://doi.org/10.61615/JMCCR/2026/MAR027140326
Copyright: © 2026 Fatta Gafar Oglu Sadikhov. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
DOI: https://doi.org/10.61615/JMCCR/2026/MAR027140326
Publication History
Received Date
16 Feb ,2026
Accepted Date
26 Feb ,2026
Published Date
26 Mar ,2026
Abstract
Background
The aim of the study is to improve the results of surgical treatment of patients with complicated forms of autoimmune thyroiditis through the introduction of advanced surgical techniques and CO2 laser in surgical interventions.
Methods
The immediate results of surgical treatment of patients with complicated forms of autoimmune thyroiditis treated at the clinical base of the Scientific Center of Surgery named after M.A. Topchubashov from 2015 to 2024 were studied. The analysis was carried out on 207 operated patients divided into two groups. The first group consisted of 96 (46.4%) patients who underwent an improved surgical technique using a CO2 laser. The second group included 111 (53.6%) patients who underwent surgery using traditional methods. The immediate postoperative results of the surgical treatment of patients in two groups were compared. To test the statistical significance of differences, nonparametric Pearson's χ2 and Student's t tests were used. Differences were considered statistically significant at p<0.050.
Results
The immediate postoperative treatment results of patients with specific and non-specific complications that arose in groups were studied. The complication rate in the first group (3.1%, n=3) was four times lower than that of the second group (14.4%, n=16) (χ2= 7.870, p=0.006, p<0.050).
Conclusion
The greatest number of complications was noted in patients with large goiters and recurrence of the disease in those previously operated on for autoimmune thyroiditis. Thus, the use of CO2 laser, along with improved surgical techniques, in thyroid surgery has an absolute advantage over the use of traditional surgical techniques.
Keywords: autoimmune thyroiditis; subtotal resection of the thyroid gland; extreme subtotal resection of the thyroid gland; thyroidectomy.
►Results of Surgical Treatment of Complicated Forms of Autoimmune Thyroiditis
Fatta Gafar Oglu Sadikhov1*
1*Scientific Center of Surgery named after M.A. Topchubashov, Baku, Azerbaijan.
Introduction
Immediate postoperative complications in the surgical treatment of autoimmune thyroiditis (AIT) occur in 1.5% to 12.0% of the total number of operated patients [1]. The incidence of autoimmune thyroiditis is up to 40%, and relapse in AIT is observed in 20%-45% [2]. Depending on clinical and laboratory studies and morphological data, various types of surgical interventions are used [3, 4]. Currently, the majority of endocrinologists agree with the opinion on the urgent need to develop new approaches to the treatment of patients with autoimmune thyroiditis, capable of significantly improving outcomes, reducing treatment costs, and decreasing patient disability rates [5, 6].
The main indications for surgical treatment of AIT are: nodular transformation of the thyroid gland (TG) with suspected development of thyroid cancer against the background of autoimmune thyroiditis and the presence of a large goiter with signs of compression of the trachea and esophagus [7]. To date, the issue of choosing the optimal extent of surgical intervention for AIT remains unresolved. Various surgical options are discussed, ranging from hemithyroidectomy to subtotal resection of the thyroid gland and even its extirpation [8].
In recent years, surgical interventions have become less common in the treatment of AIT [9]. This is primarily due to the unsatisfactory long-term results of surgical interventions for this condition. Surgical interventions resulted in improvement in only 20% of patients [10]. This effect was achieved only in patients with clinical signs of hyperthyroidism and compression of the neck organs. This is likely why some authors believe that indications for surgical intervention should be limited [11, 12].
The reserved attitude of surgeons and endocrinologists towards the surgical treatment of AIT is due to modern concepts regarding the etiopathogenesis of the disease [13]. Surgeries for AIT in most cases are technically difficult, often accompanied by complications during surgery and in the early postoperative period [13, 14]. Techniques for isolating and resecting the thyroid gland play an important role in performing surgery for AIT, since compliance with a number of conditions and rules allows for a favorable outcome in treatment and ensures a good quality of life for the patient after surgical treatment [15, 16].
The diversity of clinical variants of autoimmune thyroid diseases, the lack of a generally accepted morphological classification of the disease, the frequently atypical symptoms of the disease, and its early stage are predictors of diagnostic errors and inappropriate treatment strategies [17]. Thus, the increasing incidence of AIT, the difficulties and high percentage of immediate postoperative complications during surgical treatment, and the conflicting opinions regarding approaches to choosing a surgical strategy for patients with complicated forms of autoimmune thyroiditis indicate the relevance of this problem. In this regard, surgeons have a justified need to improve surgical tactics aimed at improving the results of surgical treatment.
The Aim of the study is to improve the results of surgical treatment of patients with complicated forms of autoimmune thyroiditis through the introduction of advanced surgical techniques and CO2 laser in surgical interventions.
Methods
This study examined the immediate postoperative outcomes of surgical treatment of patients with autoimmune thyroiditis at the clinical site of the Scientific Center of Surgery named after M.A. Topchubashov from 2015 to 2024. A total of 207 patients aged 27 to 73 years, primarily with the hypertrophic form of AIT, were operated on. There were 183 women (88.4%) and 24 men (11.6%). A surgical treatment strategy was chosen due to the complicated course of this form of AIT, characterized by growth and enlargement of the thyroid gland with the formation of a nodular or multinodular goiter, or suspected thyroid cancer. The analysis was conducted in two groups of operated patients. The first group consisted of 96 patients (46.4%) who underwent an improved surgical technique using a CO2 laser as a tool facilitating surgical intervention (a Lancet-2 CO2 laser generator; λ = 1.06 nm, Russia was used). The second group included 111 patients (53.6%) who underwent surgery using traditional methods. Immediate postoperative (during and within one month after surgery) results were compared between the two groups of patients. Immediate postoperative complications were assessed: wound bleeding, unilateral or bilateral recurrent laryngeal nerve paresis, wound suppuration, and hypoparathyroidism.
The CO2 laser is the first surgical laser and has been actively used since the 1980s. Its high absorption in water and organic compounds (penetration depth of 0.1 mm) makes the CO2 laser suitable for a wide range of surgical procedures, including thyroid surgery. The laser's surface action allows for tissue excision without causing deep damage.
In patients with AIT, the extent of surgery varied from subtotal resection to extremely subtotal thyroid resection and thyroidectomy. The surgeries complied with the recommendations of the American Association of Clinical Endocrinology, 2016, [18] and the Russian Association of Endocrinologists, 2016 [19]. Data from preoperative examination (ultrasound, cytomorphology) and pathohistological examination of the removed thyroid tissue were analyzed. The laboratory examination algorithm for patients with AIT included traditional tests: complete blood count, general urine analysis, blood biochemistry, hemo and coagulogram, and blood electrolytes. Thyroid status and the level of autoantibodies to antigenic structures of thyroid tissue were determined by measuring the concentration of thyroid hormones (free T3, free T4), pituitary hormone (TTH), and thyroid tissue antibodies (Anti-TG, Anti-TPO) in the patients' blood serum using an enzyme immunoassay.
Informed Consent: All patients signed informed consent to participate in the study.
Ethics Committee Approval: The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Scientific Center of Surgery named after M.A. Topchubashov (Minutes № 2, dated May 16, 2019).
All calculations were performed on an Excel 2019 spreadsheet. Statistical analysis was performed using IBM SPSS Statistics version 26. For each patient group, the mean values of the analyzed clinical parameters, their standard error (±m), and the reliability of intergroup differences were calculated using the χ2 and Student's t tests. Differences were considered statistically significant at p < 0.050.
Results
The early results of surgical treatment of 207 patients operated on for various forms of autoimmune thyroiditis were analyzed in two groups of patients. In order to improve the results of surgical treatment, an improved hydraulic dissection method using CO2 laser beams was applied to group I patients during surgical interventions on the thyroid gland. Due to the liquid, the local effect of the laser is easier dissection of tissues without causing deep burns. This group included 96 (46.4%) patients who underwent surgery.
Group II consisted of 111 (53.6%) patients operated on using traditional surgical methods. Conventional surgical methods and standard conventional postoperative management were used during thyroid surgery in these patients. A comparative analysis of intraoperative and early postoperative complications (within one month after surgery) was performed in two groups of patients. The following early postoperative complications were evaluated: wound bleeding, unilateral or bilateral paresis of the recurrent laryngeal nerve, wound suppuration, and hypoparathyroidism (Table 1).
Table 1. Intraoperative and Early Postoperative Complications in Two Groups of Patients Operated on for Autoimmune Thyroiditis
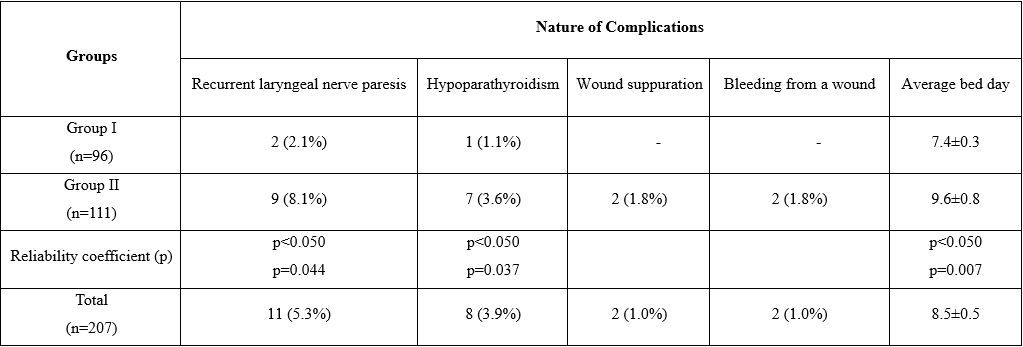
Note: Quantitative values of p>0.050 are not statistically significant
Quantitative values of p˂0.050 are statistically significant
According to the data given in Table 1, the frequency of complications in group I patients (3) is more than 5 times lower than the same indicators of group II patients (16) (χ2=7.870, p=0.006, р<0.050). The indicators of the average bed day are also 22% lower in group I patients (t=2.588, p=0.007, p˂0.050 there is a statistically significant difference). In the compared groups, a statistical difference was observed between patients with complications in the form of laryngeal paresis (χ2=4.057, р=0.044, р<0.050), a statistical difference was also observed in complications in the form of hypoparathyroidism (χ2=4.381, р=0.037, р<0.050).
All patients were divided into three age groups: the first group - 24 (11.6%) patients with an average age of 32.0 [27.0-35.0]; the second group - 118 (57.0%) patients with an average age of 51.0 [36.0-59.0] years; the third group - 65 (31.4%) patients with an average age 69.0 [60.0-74.0] years (Table 2).
Table 2. The Number of Two Groups of Patients with Autoimmune Thyroiditis Who Underwent Surgery in Different Age Groups (absolutely and in %)
|
Groups |
Young and middle-aged patients 27-59 years old |
Elderly patients 60-74 years old |
Total |
|
Group I (n=96) |
33 (34.4%) |
63 (65.6%) |
96(46.4%) |
|
Group II (n=111) |
50 (45.1%) |
61 (54.9%) |
111 (53.6%) |
|
Reliability coefficient (р) |
р>0.050 р=0.570 |
р>0.050 р=0.570 |
|
|
Total (n=207) |
83 (40.1%) |
124(59.9%) |
207 (100%) |
Note: Quantitative values of p>0.050 are not statistically significant
Table 2 shows the number of patients operated on among patients with autoimmune thyroiditis in different age groups. The data allow us to note that 124 of 207 patients (59.9%) were elderly people. There are no statistically significant differences between the number of young and middle-aged patients, as well as the number of elderly patients in groups I and II (χ2=2.454, χ2=2.449, p≈0.570, p>0.050, respectively). Taking into account different forms of autoimmune thyroiditis, we have compared the characteristics of two groups of operated patients (Table 3).
Table 3. Characteristics of Two Groups of Patients Operated on with Different Forms of Autoimmune Thyroiditis
|
Groups |
Forms of AIT |
Total
|
||
|
Diffuse-nodular |
Diffuse-pseudo nodular |
Relapse |
||
|
Group I (n=96) |
46 (47.9%) |
35** (36.5%) |
15* (15.6%) |
96 (100%) |
|
Group II (n=111) |
60 (54.0%) |
20** (18.0%) |
31* (28.0%) |
111 (100%) |
|
Reliability coefficient (р) |
p>0.050 р=0.418 |
p˂0.010 р=0.002 |
р˂0.05 р=0.034 |
|
|
Total (n=207) |
106 (51.2%) |
55 (26.6%) |
46 (22.2%) |
207 (100%) |
Note: * р˂0.050, ** р˂0.010 indicators of statistical differences
106 (51.2%) of the operated patients had diffuse-nodular; 55 (26.5%) - with a diffuse-pseudonodular form of AIT; 46 (22.2%) patients were re-operated with AIT recurrence. The statistical difference between the number of patients with diffuse-nodular and diffuse-pseudonodular forms of AIT in groups I and II was χ2emp.=0.798, р=0.418, p>0.050 and χ2emp.=8.947, р=0.002, p˂0.010, respectively. A statistically significant difference was observed between the number of patients with a recurrent form of AIT in groups I and II (χ2emp.=4.459, р=0.034, р˂0.05).
We investigated the complications encountered in the early postoperative period of 207 operated patients. In order to compare the early results of surgical interventions using the improved surgical method and CO2 laser, we examined the indicators of intraoperative blood loss and duration of surgery between group I and II patients (Table 4).
Table 4. Comparison of Indicators of Intraoperative Blood Loss and Duration of Surgery in Two Groups of Patients
|
Groups |
Intraoperative blood loss (ml) |
Duration of operation (min.) |
Number of patients with complications |
Number of inpatient deaths |
|
Group I (n=96) |
172.4±37.2 |
92±23.1 |
3 (3.1%) |
1 (1.0%) |
|
Group II (n=111) |
213.0±43.4 |
104±19.7 |
16 (14.4%) |
4 (3.6%) |
|
Reliability coefficient (р) |
р>0.050 р=0.492 |
р>0.050 р=0.665 |
р<0.050 p=0.006 |
р>0.050 р=0.230 |
|
Total (n=207) |
196±40.3 |
98.0±21.4 |
19 (9.2%) |
5 (2.4%) |
Note: Quantitative values of p>0.050 are not statistically significant
Quantitative values of p˂0.050 are statistically significant
Intraoperative blood loss (t=0.710, p=0.492, p>0.050) and duration of surgery (t=0.395, p=0.665, p>0.050) were statistically significant differences between groups. A statistically significant difference was observed in the number of patients with specific complications in groups I and II (χ2=7.870, p=0.006, р<0.050). There was no statistically significant difference between the number of deaths in the hospital (χ2=1.396, p=0.230, p>0.050). Indications confirm less intraoperative blood loss and shorter operative time in group I patients.
Our comparative analysis confirms that the use of CO2 laser, along with improved surgical techniques for performing operations on the thyroid gland, has an absolute advantage over the use of traditional surgical methods. This method is applied in the presence of adhesion and fibrous changes that disrupt anatomical connections in the surgical field, which allowed to reduce the percentage of patients with laryngeal paresis (χ2=4.057, р=0.044, р<0.050) and hypoparathyroidism by four times (χ2=4.381, р=0.037, р<0.050). It helped reduce postoperative bed days by 22%, from 9.6 to 7.4 days (t=2.588, p=0.007, p˂0.050, statistically significant difference is detected).
The analysis of the early results of surgical treatment of patients with various forms of autoimmune thyroiditis gives reason to believe that the surgical treatment method shows good results despite the presence of several complications if there are clear indications for the operation and the use of modern laser technology. Therefore, with the right approaches, this method has allowed us to obtain very favorable positive results.
Discussion
Prevention of postoperative complications in patients with AIT is the responsibility of the operating surgeon [7, 9]. Currently, indications for surgical treatment of AIT have been determined; the technique and scope of surgical intervention have been developed depending on the nature and extent of thyroid damage [3, 4]. Despite this, immediate postoperative complications in the surgical treatment of autoimmune thyroiditis occur in 1.5% to 12.0% of the total number of operated patients, sometimes resulting in patient disability [1, 2]. This is confirmed by our studies. In our practice, postoperative complications developed in 8.5% of patients: bleeding - in 2 (1.0%) patients, unilateral or bilateral paresis of the recurrent laryngeal nerve - in 11 (5.3%), wound suppuration - in 2 (1.0%), hypoparathyroidism - in 8 (3.9%), and hospital mortality - 5 (2.4%) patients.
When using traditional surgical methods during thyroid surgery in patients of group II, 16 (14.4%) of 111 patients had general complications in the early postoperative period. The use of improved surgical techniques and CO2 laser during thyroid surgery in patients of group I (96 patients) reduced the total number of complications to 3 (3.1%). According to the literature, postoperative hypoparathyroidism is caused by trauma to the parathyroid glands and occurs in 1.5% to 7% of cases after thyroid surgery [1, 9, 16]. The use of improved surgical techniques and intraoperative use of CO2 laser, which allows for surgical intervention under visual control of the localization zones of the superior laryngeal nerve and parathyroid glands, and careful work of the surgeon in the area of their localization help to reduce the incidence of both unilateral and bilateral injuries.
The volume of surgery varied from subtotal resection of the thyroid gland, 69 (33.3%) patients, to extremely subtotal resection of the gland, 43 (20.8%) people, and thyroidectomy, 95 (45.9%) patients. In this regard, there is an urgent need for further research to improve the methods of surgical treatment of patients with autoimmune thyroiditis. This study revealed that the use of CO2 laser in the surgical treatment of patients with autoimmune thyroiditis leads to a four-fold decrease in the percentage of patients with complications (χ2=7.870, p=0.006, p<0.050).
We analyzed the results of the surgical treatment of patients in two groups. The first included 96 patients (46.4%) who underwent surgery using a CO2 laser as a tool during surgery and using an improved surgical technique. The second group included 111 patients (53.6%) who underwent surgery using a traditional surgical technique and standard postoperative care. The complication rate in group I patients was more than four times lower than among patients in group II. The average bed-day was also 22% lower in patients in group I (t=2.588, p=0.007, p<0.050, significant differences). Statistical processing of the obtained data confirmed significant differences in the complication rate and mortality in the two comparison groups. The percentage of patients with complications among patients in the first group (3.1%, n=3) is four times less than the number of patients with complications (14.4%, n=16) among patients in the second group (χ2=7.870, p=0.006, p<0.050, significant differences).
Thus, the conducted analysis gives grounds to believe that the use of CO2 laser, along with improved surgical techniques, in thyroid surgery has an absolute advantage over the use of traditional surgical techniques.
Conflict of Interest
The author declares no conflict of interest regarding this article.
Acknowledgments
The study received no sponsorship support. The author of the article expresses his gratitude to Rauf Magsud Oglu Agayev, for methodological assistance in conducting this study.
Conclusion
- The presence of large tumors in the thyroid gland against the background of the complications of autoimmune thyroiditis, the formation and growth of nodular or multinodular tumors, the presence of severe thyrotoxicosis, and the risk of developing a malignant neoplasm of the thyroid gland should be indications for surgical intervention. In the surgical treatment of the disease, near-total resection of the thyroid gland and thyroidectomy with the improved hydraulic dissection method using CO2 laser rays are the operations of choice.
- Application of improved hydraulic dissection method using CO2–laser rays to perform surgical operations on the thyroid gland in patients with autoimmune thyroiditis, and performing the operation in an adequate volume has an advantage over the use of traditional surgical methods (p≤0.050). This method is applied in the presence of adhesion and fibrous changes that disrupt the anatomical structure in the surgical field, which has allowed to reduce the percentage of patients with laryngeal paresis (χ2=4.057, р=0.044, р<0.050) and hypoparathyroidism by four times (χ2=4.381, р=0.037, р<0.050), reduced the postoperative bed days from 9.6 to 7.4 days (t=2.588, p=0.007, p˂0.050).
- Sadikhov FG, Agaev RM, Gardashov NT, (2021). Assessment of immediate and long-term results of treatment of patients with autoimmune thyroiditis // Bulletin of the National Medical and Surgical Center named after.N.I. Pirogova. 16(3):42-46.
- Sadikhov FG, (2023). Immediate results of surgical treatment of autoimmune thyroiditis with the introduction of improved surgical techniques // Kazan Medical Journal. 104(3):461-468.
- Antonelli A, Ferrari SM, Corrado A, Di Domenicantonio A, Fallahi P, (2013). Autoimmune thyroid disorders // Autoimmunity reviews. 2015;14(2):174-180.
- Ryabchenko EV, (2018). Features of surgical treatment of thyroid tumors in combination with chronic autoimmune thyroiditis // Scientific Bulletin of Healthcare of Kuban. 57(3):29-38.
- Alnefaie SM, (2023). Surgical decision-making in thyroiditis: a review article // Cureus. 15(9):e46055.
- Panchangam RB, Kota SK, Mayilvaganan S, Kuravi BG, (2021). What is the impact of thyroidectomy on autoimmune features associated with Hashimoto's thyroiditis?- Institutional experience // Nigerian journal of clinical practice. 24(6):905-910.
- Tsilimigras DI, Patrini D, Antonopoulou A, Velissaris D, Koletsis E, Lawrence D. (2017). Retrosternal goitre: the role of the thoracic surgeon // Journal of thoracic disease. 9(3):860-863.
- Guldvog I, Reitsma LC, Johnsen L, Lauzike A, Gibbs C, Carlsen E. (2019). Thyroidectomy versus medical management for euthyroid patients with Hashimoto disease and persisting symptoms: a randomized trial // Annals of internal medicine. 170(7):453-464.
- Heggie K, Yeung M, Grodski S, Lee J, Serpell J, (2018). Total thyroidectomy for pressure symptoms in patients with Hashimoto's thyroiditis // ANZ journal of surgery. 88(4):359-362.
- Peng CC, Munir KM, Song L, Papadimitriou JC, Pennant MA, (2020). Recurrent painful Hashimoto thyroiditis successfully treated by thyroidectomy // AACE clinical case reports. 6(1):e9-13.
- Gan T, Randle RW, (2019). The role of surgery in autoimmune conditions of the thyroid // Surgical clinics of north America. 99(4):633-648.
- Berber E, Bernet V, Fahey TJ 3rd, Kebebew E, Shaha A, Stack BC Jr, (2016). American Thyroid Association statement on remote-access thyroid surgery // Thyroid. 26(3):331-337.
- Zivaljevic VR, Bukvic Bacotic BR, Sipetic SB, Stanisavljevic DM, Maksimovic JM, Diklic AD, (2015). Quality of life improvement in patients with Hashimoto thyroiditis and other goiters after surgery: a prospective cohort study // International journal of surgery (London, England). (21):150-155.
- Krakovitz P, Cairns C, Schweiger BM, Burkey B, (2018). Surgical management of neck pain and headache associated with pediatric Hashimoto's thyroiditis // Laryngoscope. 128(9):2213-2217.
- Boutzios G, Tsourouflis G, Garoufalia Z, Alexandraki K, Kouraklis G, (2019). Long-term sequelae of the less than total thyroidectomy procedures for benign thyroid nodular disease // Endocrine. 63(2):247-250.
- Nawarathna NJ, Ratnayake P, Hewage SN, Senevirathne R Jk, Gunatilake SSc, Kariyawasam NL, (2018). Association between nonspecific chronic lymphocytic thyroiditis and differentiated epithelial thyroid carcinoma: clinicopathological analysis of patients who underwent thyroidectomy in a tertiary care center in Sri Lanka // World journal of endocrine surgery. 10 (2):119-126.
- Gan X, Feng J, Deng X, Shen F, Lu J, Liu Q, (2021). The significance of Hashimoto's thyroiditis for postoperative complications of thyroid surgery: a systematic review and meta-analysis // Annals of the royal college of surgeons of England. 103(3):223-230.
- Gharib H, Papini E, Garber Jr, Duick DS, Harrell RM, Hegedüs L, (2016). American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinology medical guidelines for clinical practice for the diagnosis and management of thyroid nodules – 2016 update // Endocrine practice. (22):622-639.
- Beltsevich DG, Vanushko VE, Melnichenko GA, Rumyantsev PO, Fadeev VV, (2016). Russian Association of Endocrinologists clinic guidelines for thyroid nodules diagnostic and treatment // Endocrine Surgery. 10(1):5-12.
Download Provisional PDF Here
PDF